WE ACCEPT MOST INSURANCE PROVIDERS!
WE ACCEPT MOST INSURANCE PROVIDERS!

Heart health is a cornerstone of overall well-being, but coronary artery disease (CAD) poses a significant challenge for many individuals. This narrowing of the pathways restricts the delivery of life-sustaining oxygen to the heart muscle. If you're navigating the complexities of CAD, exploring treatment options such as coronary balloon angioplasty can be a transformative step towards reclaiming your heart's vitality and ensuring a brighter, healthier future. Residents in the area are welcomed to call Capitol Cardiology Associates to schedule a consultation or appointment with a licensed cardiologist. Knowledgeable members of our team are on standby to address questions or concerns you may have.
Coronary arteries, essential for optimal heart function, can become restricted due to plaque buildup. This can lead to symptoms like chest pain (angina) or even increase the risk of heart attack.
Coronary balloon angioplasty, also known as percutaneous transluminal coronary angioplasty (PTCA), is a minimally invasive procedure designed to open narrowed or blocked coronary arteries.
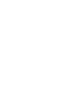
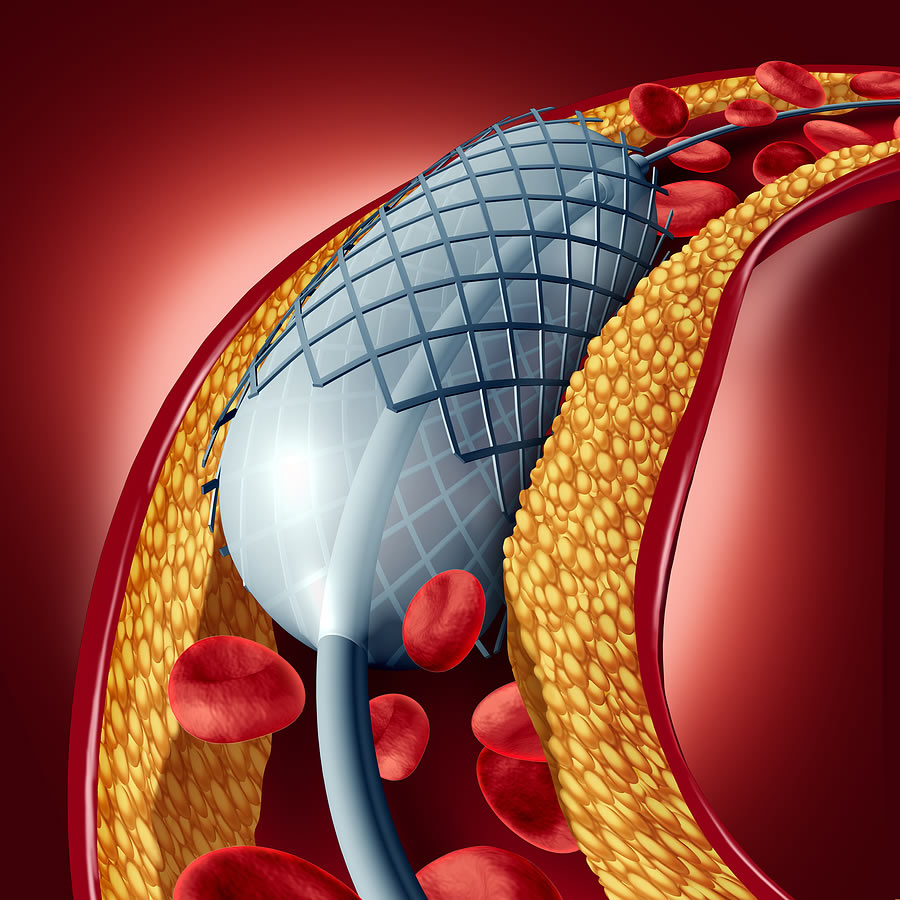
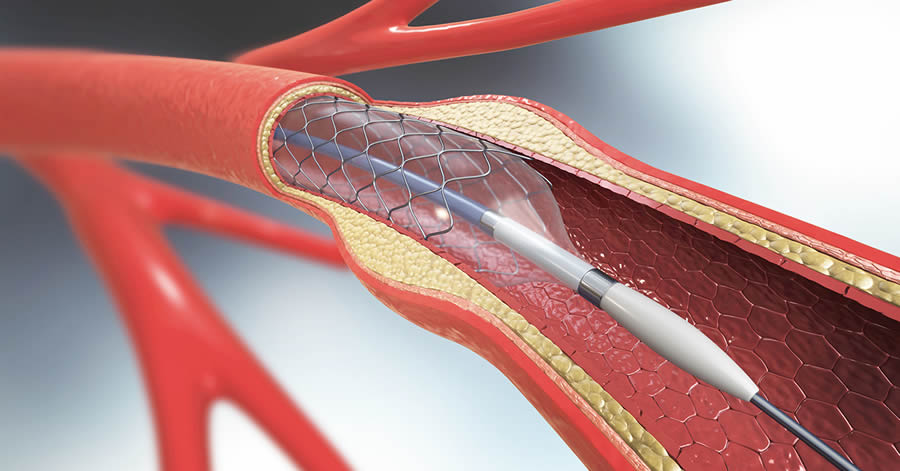
The procedure involves a specialized catheter equipped with a deflated balloon. Guided by advanced imaging technology, the catheter is gently threaded through an artery – typically in the groin or wrist – until it reaches the affected coronary artery segment.
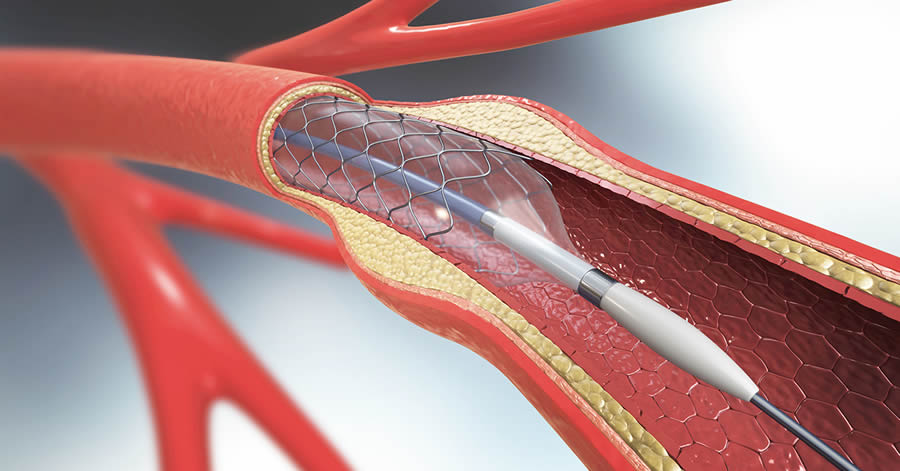
Once in position, the balloon is inflated, exerting gentle pressure against the artery walls and compressing the plaque, thereby widening the artery and restoring proper blood flow.
In some cases, a stent (a small mesh-like tube) may be placed during the procedure to help keep the artery open and prevent re-narrowing.
By opening narrowed or blocked arteries, angioplasty relieves symptoms such as chest pain, shortness of breath, and fatigue, enhancing overall heart function and quality of life. Placing a stent during angioplasty helps maintain the patency of the treated artery over time and reduces the risk of re-narrowing.
Compared to traditional open-heart surgery, angioplasty is minimally invasive, resulting in shorter recovery times, reduced hospital stays, and a quicker return to daily activities. Angioplasty is even associated with lower complication rates compared to more invasive surgical interventions, offering a safer option for many individuals with CAD.
At Capitol Cardiology Associates, each angioplasty procedure is tailored to our patient's specific needs. We take pride in providing personalized care and optimal outcomes.


Your cardiologist or physician may recommend coronary balloon angioplasty for you if you:
Individual cases vary, and it is important to consult with your physician and even seek a second opinion before making a decision. Residents in the area are welcomed to call Capitol Cardiology Associates to schedule a phone consultation, face-to-face meeting, or an appointment for a convenient time. Our team is here to take your call or message today.